Couldn't find a graph in English. Apologies. Here's an article on UBT251 -> https://www.fiercebiotech.com/biote...triple-g-agonist-tied-15-weight-loss-12-weeks


quoted said:An experimental, triple-acting obesity drug from Novo Nordisk helped some patients in a Phase 2 trial in China lose up to a fifth of their body weight , the company said Tuesday.
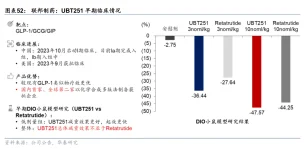
The study, run by Novo’s Guangdong, China-based development partner United Biotechnology, enrolled 205 patients who are overweight or have obesity and tested three different doses of the therapy, UBT251 , against a placebo over 24 weeks . According to Novo, the highest average weight loss observed over that time was 19.7% , versus 2% for placebo recipients.
Novo didn’t provide other details, but said all dose groups had statistically significant improvements compared to a placebo on key secondary measures of metabolic health. The most common side effects were gastrointestinal in nature and the “vast majority” were mild to moderate and diminished over time, the company said. Initial data from a global Phase 1b/2a study are expected next year...
In a mid-stage study published in The New England Journal of Medicine three years ago, retatrutide treatment led to as much as 17.5% weight loss after 24 weeks . Without mentioning retatrutide by name, Martin Holst Lange, Novo’s chief scientific officer and research head, claimed in a statement Tuesday that UBT251’s results suggest a “differentiated” clinical, safety and tolerability profile.

Yeah, saner prices in AUS maybe. The best one gets the golden ring in the USA.lessthanhalf said:The more new drugs the better. I think a lot of the drugs that have been in development that are injectable and not triple agonists will end up being dropped, as they won't compete with reta or any of the other ones being worked out. But over the longer term the more drugs the more competition and eventually saner pricing. The holy grail would be an oral triple agonist but I have not heard of one yet.
This one sounds very good, and unless something goes wrong, will keep going. You really need to know the incidence of side effects vs weight loss to compare drugs, as otherwise just giving a bit higher dose is going to make that drug look more effective, even if it causes more nausea or vomiting .
If we are whipping out who has the biggest weight loss drugs Why settle for nn-9559 or UBT-251 when you can look forward to NA-931fatbegone said:Couldn't find a graph in English. Apologies. Here's an article on UBT251 -> https://www.fiercebiotech.com/biote...triple-g-agonist-tied-15-weight-loss-12-weeks
View attachment 6479
I got to hand it to the Chinese, One things is they do have plenty of willing volunteers ( Uyghurs ) to preform these trials on the population.lessthanhalf said:Sadly it is not a peptide and as far as I know the chemical structure is not published so no pirate Chinese versions in the near future.
Big pharma finally catching up to bro science.DjJoshua said:If we are whipping out who has the biggest weight loss drugs Why settle for nn-9559 or UBT-251 when you can look forward to NA-931
What NA-931 TargetsIt's a first-in-class, oral small-molecule quadruple agonist that simultaneously activates:
GLP-1 (appetite suppression, glucose control)
GIP (insulin sensitivity, fat metabolism)
Glucagon (energy expenditure, fat burning)
IGF-1 (insulin-like growth factor-1, which supports muscle growth , repair, and lean mass preservation)
The key differentiator here is the IGF-1 component—IGF-1 pathways help counteract the catabolic (muscle-breaking) effects common with GLP-1-based drugs, where 15–40% of weight loss can come from lean mass (especially concerning at age 52+ for sarcopenia risk).
Except that it's pretty well understood to be vaporware which will never exist in the world of the realDjJoshua said:when you can look forward to NA-931
How about a 100% non glp1..... look at this.. The Allurion Gastric Balloon (also known as the Allurion Balloon or previously the Elipse Balloon in earlier studies). It's a swallowable intragastric balloon designed for non-surgical weight loss.Calm Logic said:Big pharma finally catching up to bro science.